PROFESSOR DR. NUMAN NAFIE HAMEED الاستاذ الدكتور نعمان نافع الحمداني
|
|
|
- Abel Walker
- 5 years ago
- Views:
Transcription
1 Lecture 6 PROFESSOR DR. NUMAN NAFIE HAMEED الاستاذ الدكتور نعمان نافع الحمداني Neonatal Resuscitation Program (NRP) 2010 MCQ? In neonatal resuscitation program, the preterm neonates need special preparations because they have all the following Except: a. Preterm babies also have immature blood vessels in the brain that are prone to hemorrhage b. Have no susceptibility to infection c. They are also more vulnerable to injury by positive-pressure ventilation. d. increased risk of hypovolemic shock related to small blood volume e. thin skin and a large surface area, which contribute to rapid heat loss Approximately 10% of newborns require some assistance to begin breathing at birth. Less than 1% requires extensive resuscitative measures. Although the vast majority of newly born infants do not require intervention to make the transition from intrauterine to extrauterine life, because of the large total number of births, a sizable number will require some degree of resuscitation. Those newly born infants who do not require resuscitation can generally be identified by a rapid assessment of the following 3 characteristics: Term gestation? Crying or breathing? Good muscle tone? If the answer to all 3 of these questions is yes, the baby does not need resuscitation and should not be separated from the mother. The baby should be dried, placed skin-to-skin with the mother, and covered with dry linen to maintain temperature. Observation of breathing, activity, and color should be ongoing. If the answer to any of these assessment questions is no, the infant should receive one or more of the following 4 categories of action in sequence: A. Initial steps in stabilization (provide warmth, clear airway if necessary, dry, stimulate) B. Ventilation C. Chest compressions D. Administration of epinephrine and/or volume expansion 1
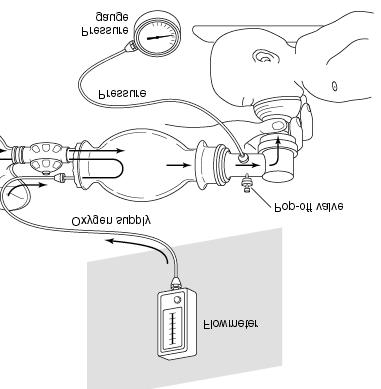
2 Approximately 60 seconds ( the Golden Minute ) are allotted for completing the initial steps, reevaluating, and beginning ventilation if required. The decision to progress beyond the initial steps is determined by simultaneous assessment of 2 vital characteristics: respirations (apnea, gasping, or labored or unlabored breathing) and heart rate (whether greater than or less than 100 beats per minute). Assessment of heart rate should be done by intermittently auscultating the precordial pulse. When a pulse is detectable, palpation of the umbilical pulse can also provide a rapid estimate of the pulse. A pulse oximeter can provide a continuous assessment of the pulse without interruption of other resuscitation measures. Once positive pressure ventilation or supplementary oxygen administration is begun, assessment should consist of simultaneous evaluation of 3 vital characteristics: heart rate, respirations, and the state of oxygenation, the latter optimally determined by a pulse oximeter. The most sensitive indicator of a successful response to each step is an increase in heart rate. Anticipation of Resuscitation Need At every delivery there should be at least one person whose primary responsibility is the newly born. This person must be capable of initiating resuscitation, including administration of positive-pressure ventilation and chest compressions. Either that person or someone else who is promptly available should have the skills required to perform a complete resuscitation, including endotracheal intubation and administration of medications. With careful consideration of risk factors, the majority of newborns who will need resuscitation can be identified before birth. If a preterm delivery (37 weeks of gestation) is expected, special preparations will be required because: 1. Preterm babies have immature lungs that may be more difficult to ventilate and are also more vulnerable to injury by positive-pressure ventilation 2. Preterm babies also have immature blood vessels in the brain that are prone to hemorrhage 3. Thin skin and a large surface area, which contribute to rapid heat loss 4. increased susceptibility to infection 5. Increased risk of hypovolemic shock related to small blood volume. Initial Steps The initial steps of resuscitation are to provide warmth by placing the baby under a radiant heat source, positioning the head in a sniffing position to open the airway, clearing the airway if necessary with a bulb syringe or suction catheter, drying the baby, and stimulating breathing. 2
3 Temperature Control Very low-birth-weight (<1500 g) preterm babies are likely to become hypothermic despite the use of traditional techniques for decreasing heat loss. additional warming techniques are recommended (eg. prewarming the delivery room to 26 C, covering the baby in plastic wrapping, placing the baby on an exothermic mattress, and placing the baby under radiant heat. The infant s temperature must be monitored closely. Other techniques for maintaining temperature during stabilization (eg, prewarming the linen, drying and swaddling, placing the baby skin-to-skin with the mother and covering both with a blanket) are recommended. All resuscitation procedures, including endotracheal intubation, chest compression, and insertion of intravenous lines, can be performed with these temperature-controlling interventions in place. Infants born to febrile mothers have been reported to have a higher incidence of perinatal respiratory depression, neonatal seizures, and cerebral palsy and an increased risk of mortality. Hyperthermia should be avoided. The goal is to achieve normothermia and avoid iatrogenic hyperthermia. Clearing the Airway When Amniotic Fluid Is Clear There is evidence that suctioning of the nasopharynx can create bradycardia during resuscitation and that suctioning of the trachea in intubated babies receiving mechanical ventilation in the neonatal intensive care unit (NICU) can be associated with deterioration of pulmonary compliance and oxygenation and reduction in cerebral blood flow velocity when performed routinely (ie, in the absence of obvious nasal or oral secretions). However, there is also evidence that suctioning in the presence of secretions can decrease respiratory resistance. Therefore it is recommended that suctioning immediately following birth should be reserved for babies who have obvious obstruction to spontaneous breathing or who require positive-pressure ventilation (PPV). When Meconium is Present Aspiration of meconium before delivery, during birth, or during resuscitation can cause severe meconium aspiration syndrome (MAS). In the absence of randomized, controlled trials, there is insufficient evidence to recommend a change in the current practice of performing endotracheal suctioning of nonvigorous babies with meconium-stained amniotic fluid. However, if attempted intubation is prolonged and unsuccessful, bag-mask ventilation should be considered, particularly if there is persistent bradycardia. Assessment of Oxygen Need and Administration of Oxygen Blood oxygen levels in uncompromised babies generally do not reach extrauterine values until approximately 10 minutes following birth. Oxyhemoglobin saturation 3
4 may normally remain in the 70% to 80% range for several minutes following birth, thus resulting in the appearance of cyanosis during that time. Pulse Oximetry It is recommended that oximetry be used when 1. Resuscitation can be anticipated, 2. When positive pressure is administered for more than a few breaths, 3. When cyanosis is persistent, 4. Or when supplementary oxygen is administered Administration of Supplementary Oxygen It is recommended that the goal in babies being resuscitated at birth, whether born at term or preterm, should be an oxygen saturation value in the interquartile range of preductal saturations measured in healthy term babies following vaginal birth at sea level. These targets may be achieved by initiating resuscitation with air or a blended oxygen and titrating the oxygen concentration to achieve an SpO2 in the target range. If blended oxygen is not available, resuscitation should be initiated with air. If the baby is bradycardic (HR <60 per minute) after 90 seconds of resuscitation with a lower concentration of oxygen, oxygen concentration should be increased to 100% until recovery of a normal heart rate. Positive-Pressure Ventilation (PPV) If the infant remains apneic or gasping, or if the heart rate remains <100 per minute after administering the initial steps, start PPV. Initial Breaths and Assisted Ventilation Assisted ventilation should be delivered at a rate of 40 to 60 breaths per minute to promptly achieve or maintain a heart rate>100 per minute. End-Expiratory Pressure Many experts recommend administration of continuous positive airway pressure (CPAP) to infants who are breathing spontaneously, but with difficulty, following birth. Starting infants on CPAP reduced the rates of intubation and mechanical ventilation, surfactant use, and duration of ventilation, but increased the rate of pneumothorax. 4
5 Spontaneously breathing preterm infants who have respiratory distress may be supported with CPAP or with intubation and mechanical ventilation. Nevertheless, PEEP is likely to be beneficial and should be used if suitable equipment is available. PEEP can easily be given with a flow-inflating bag or T- piece resuscitator. Assisted-Ventilation Devices Effective ventilation can be achieved with either a flow inflating or self-inflating bag or with a T-piece mechanical device designed to regulate pressure. Laryngeal Mask Airways Laryngeal mask airways that fit over the laryngeal inlet have been shown to be effective for ventilating newborns weighing more than 2000 g or delivered>34 weeks gestation. There are limited data on the use of these devices in small preterm infants, ie, <2000 g or <34 weeks. A laryngeal mask should be considered during resuscitation if facemask ventilation is unsuccessful and tracheal intubation is unsuccessful or not feasible. The laryngeal mask airway (LMA) is used in various clinical scenarios, including the followings: a. In neonatal resuscitation of term and large > 34 weeks preterm babies b. In the difficult airway, such as in the Robin sequence c. As an aid to endotracheal intubation d. As an aid in flexible endoscopy e. In surgical cases in place of endotracheal intubation Endotracheal Tube Placement Endotracheal intubation may be indicated at several points during neonatal resuscitation: Initial endotracheal suctioning of non-vigorous meconium stained newborns If bag-mask ventilation is ineffective or prolonged When chest compressions are performed For special resuscitation circumstances, such as congenital diaphragmatic hernia or extremely low birth weight. The timing of endotracheal intubation may also depend on the skill and experience of the available providers. After endotracheal intubation and administration of intermittent positive pressure, a prompt increase in heart rate is the best indicator that the tube is in the tracheobronchial tree and providing effective ventilation. Exhaled CO2 detection is effective for confirmation of endotracheal tube placement in infants, including very low-birth-weight infants. 5
6 Other clinical indicators of correct endotracheal tube placement are condensation in the endotracheal tube, chest movement, and presence of equal breath sounds bilaterally. Chest Compressions Chest compressions are indicated for a heart rate that is<60 per minute despite adequate ventilation with supplementary oxygen for 30 seconds. Because ventilation is the most effective action in neonatal resuscitation and because chest compressions are likely to compete with effective ventilation, rescuers should ensure that assisted ventilation is being delivered optimally before starting chest compressions. Compressions should be delivered on the lower third of the sternum to a depth of approximately one third of the anterior-posterior diameter of the chest. Two techniques have been described: compression with 2 thumbs with fingers encircling the chest and supporting the back (the 2 thumb encircling hands technique) or compression with 2 fingers with a second hand supporting the back. the 2 thumb encircling hands technique is recommended for performing chest compressions in newly born infants. Compressions and ventilations should be coordinated to avoid simultaneous delivery. The chest should be permitted to reexpand fully during relaxation, but the rescuer s thumbs should not leave the chest. There should be a 3:1 ratio of compressions to ventilations with 90 compressions and 30 breaths to achieve approximately 120 events per minute to maximize ventilation at an achievable rate. It is recommended that a 3:1 ratio be used for neonatal resuscitation where compromise of ventilation is nearly always the primary cause, but rescuers should consider using higher ratios (eg, 15:2) if the arrest is believed to be of cardiac origin. Respirations, heart rate, and oxygenation should be reassessed periodically, and coordinated chest compressions and ventilations should continue until the spontaneous heart rate is>60/ min. Medications Drugs are rarely indicated in resuscitation of the newly born infant. Bradycardia in the newborn infant is usually the result of inadequate lung inflation or profound hypoxemia, and establishing adequate ventilation is the most important step toward correcting it. However, if the heart rate remains <60/ min. despite adequate ventilation (usually with endotracheal intubation) with 100% oxygen and chest compressions, administration of epinephrine or volume expansion, or both, may be indicated. 6
7 Rarely, buffers, a narcotic antagonist, or vasopressors may be useful after resuscitation, but these are not recommended in the delivery room. Rate and Dose of Epinephrine Administration Epinephrine is recommended to be administered intravenously. The IV route should be used as soon as venous access is established. The recommended IV dose is 0.01 to 0.03 mg/kg per dose. While access is being obtained, administration of a higher dose (0.05 to 0.1 mg/kg) through the endotracheal tube may be considered, but the safety and efficacy of this practice have not been evaluated. The concentration of epinephrine for either route should be 1:10,000 (0.1 mg/ml). Volume Expansion Volume expansion should be considered when blood loss is known or suspected (pale skin, poor perfusion, weak pulse) and the baby s heart rate has not responded adequately to other resuscitative measures. An isotonic crystalloid solution or blood is recommended for volume expansion in the delivery room. The recommended dose is 10 ml/kg, which may need to be repeated. When resuscitating premature infants, care should be taken to avoid giving volume expanders rapidly, because rapid infusions of large volumes have been associated with intra-ventricular hemorrhage. Post-resuscitation Care Babies who require resuscitation are at risk for deterioration after their vital signs have returned to normal. Once adequate ventilation and circulation have been established, the infant should be maintained in, or transferred to an environment where close monitoring and anticipatory care can be provided. Naloxone Administration of naloxone is not recommended as part of initial resuscitative efforts in the delivery room for newborns with respiratory depression. Heart rate and oxygenation should be restored by supporting ventilation. Glucose Newborns with lower blood glucose levels are at increased risk for brain injury and adverse outcomes after a hypoxic ischemic insult, although no specific glucose level associated with worse outcome has been identified. Intravenous glucose infusion should be considered as soon as practical after resuscitation, with the goal of avoiding hypoglycemia. Induced Therapeutic Hypothermia It is recommended that infants born at >36 weeks gestation with evolving moderate to severe hypoxic-ischemic encephalopathy should be offered therapeutic hypothermia. 7

8 The treatment should be implemented according to the studied protocols, which currently include commencement within 6 hours following birth, continuation for 72 hours, and slow rewarming over at least 4 hours. 8
9 9
10 Equipment Needed for Intubation Laryngoscope with premature (Miller no. 0) and infant blades (Miller no. 1); Miller no. 00 optional for extremely premature infant Batteries and extra bulbs Endotracheal tubes, sizes 2.5, 3.0, 3.5, and 4.0 mm ID Stylet Suction apparatus (wall) Suction catheters: 5.0, 6.0, 8.0, and 10.0 French Meconium aspirator Oral airway Stethoscope Non self-inflating bag (0.5 L), manometer, and tubing; self-inflating bag with reservoir, manometer optional for self-inflating bag Newborn and premature mask Source of compressed air/o 2 with capability for blending Humidification and warming apparatus for air/o 2 Tape Scissors Magill neonatal forceps Elastoplast (elastic bandages) Cardiorespiratory monitor Carbon dioxide monitor or detector Pulse oximeter (Spo 2 ) Summary of changes since 2010 guidelines The following are the main changes that have been made to the guidelines for resuscitation at birth in 2015: Support of transition: Recognising the unique situation of the baby at birth, who rarely requires resuscitation but sometimes needs medical help during the process of postnatal transition. The term support of transition has been introduced to better distinguish between interventions that are needed to restore vital organ functions (resuscitation) or to support transition. Cord clamping: For uncompromised babies, a delay in cord clamping of at least 1 min from the complete delivery of the infant, is now recommended for term and preterm babies. As yet there is insufficient evidence to recommend an appropriate time for clamping the cord in babies who require resuscitation at birth.
11 Temperature: The temperature of newly born non-asphyxiated infants should be maintained between 36.5 C and 37.5 C after birth. The importance of achieving this has been highlighted and reinforced because of the strong association with mortality and morbidity. The admission temperature should be recorded as a predictor of outcomes as well as a quality indicator. Maintenance of temperature: At <32 weeks gestation, a combination of interventions may be required to maintain the temperature between 36.5 C and 37.5 C after delivery through admission and stabilisation. These may include warmed humidified respiratory gases, increased room temperature plus plastic wrapping of body and head, plus thermal mattress or a thermal mattress alone, all of which have been effective in reducing hypothermia. Optimal assessment of heart rate: It is suggested in babies requiring resuscitation that the ECG can be used to provide a rapid and accurate estimation of heart rate. Meconium: Tracheal intubation should not be routine in the presence of meconium and should only be performed for suspected tracheal obstruction. The emphasis should be on initiating ventilation within the first minute of life in non-breathing or ineffectively breathing infants and this should not be delayed. Air/Oxygen: Ventilatory support of term infants should start with air. For preterm infants, either air or a low concentration of oxygen (up to 30%) should be used initially. If, despite effective ventilation, oxygenation (ideally guided by oximetry) remains unacceptable, use of a higher concentration of oxygen should be considered. Continuous Positive Airways Pressure (CPAP): Initial respiratory support of spontaneously breathing preterm infants with respiratory distress may be provided by CPAP rather than intubation 11
Neonatal Life Support Provider (NLSP) Certification Preparatory Materials
 Certification Preparatory Materials") Neonatal Life Support Provider (NLSP) Certification Preparatory Materials NEONATAL LIFE SUPPORT PROVIDER (NRP) CERTIFICATION TABLE OF CONTENTS NEONATAL FLOW ALGORITHM.2 INTRODUCTION 3 ANTICIPATION OF RESUSCITATION
Neonatal Life Support Provider (NLSP) Certification Preparatory Materials NEONATAL LIFE SUPPORT PROVIDER (NRP) CERTIFICATION TABLE OF CONTENTS NEONATAL FLOW ALGORITHM.2 INTRODUCTION 3 ANTICIPATION OF RESUSCITATION
 NEONATAL LIFE SUPPORT PROVIDER (NLSP) CERTIFICATION EXAMINATION 1. To determine if an infant requires resuscitation, you must rapidly assess gestation period, presence of meconium in amniotic fluid, breaths
NEONATAL LIFE SUPPORT PROVIDER (NLSP) CERTIFICATION EXAMINATION 1. To determine if an infant requires resuscitation, you must rapidly assess gestation period, presence of meconium in amniotic fluid, breaths
Table 1: The major changes in AHA / AAP neonatal resuscitation guidelines2010 compared to previous recommendations in 2005
 Table 1: The major changes in AHA / AAP neonatal guidelines2010 compared to previous recommendations in 2005 Resuscitation step Recommendations (2005) Recommendations (2010) Comments/LOE 1) Assessment
Table 1: The major changes in AHA / AAP neonatal guidelines2010 compared to previous recommendations in 2005 Resuscitation step Recommendations (2005) Recommendations (2010) Comments/LOE 1) Assessment
Addendum to the NRP Provider Textbook 6 th Edition Recommendations for specific modifications in the Canadian context
 Addendum to the NRP Provider Textbook 6 th Edition Recommendations for specific modifications in the Canadian context A subcommittee of the Canadian Neonatal Resuscitation Program (NRP) Steering Committee
Addendum to the NRP Provider Textbook 6 th Edition Recommendations for specific modifications in the Canadian context A subcommittee of the Canadian Neonatal Resuscitation Program (NRP) Steering Committee
5 Million neonatal deaths each year worldwide. 20% caused by neonatal asphyxia. Improvement of the outcome of 1 million newborns every year
 1 5 Million neonatal deaths each year worldwide 20% caused by neonatal asphyxia Improvement of the outcome of 1 million newborns every year International Liaison Committee on Resuscitation (ILCOR) American
1 5 Million neonatal deaths each year worldwide 20% caused by neonatal asphyxia Improvement of the outcome of 1 million newborns every year International Liaison Committee on Resuscitation (ILCOR) American
Equipment: NRP algorithm, MRSOPA table, medication chart, SpO 2 table Warm
 NRP Skills Stations Performance Skills Station OR Integrated Skills Station STATION: Assisting with and insertion of endotracheal tube (ETT) Equipment: NRP algorithm, MRSOPA table, medication chart, SpO
NRP Skills Stations Performance Skills Station OR Integrated Skills Station STATION: Assisting with and insertion of endotracheal tube (ETT) Equipment: NRP algorithm, MRSOPA table, medication chart, SpO
NRP Raising the Bar for Providers and Instructors
 NRP 2011 Raising the Bar for Providers and Instructors What is the same? 1. Minimum course requirement is Lessons 1 through 4 and Lesson 9. The NRP Provider Card requires renewal every 2 years. Your facility
NRP 2011 Raising the Bar for Providers and Instructors What is the same? 1. Minimum course requirement is Lessons 1 through 4 and Lesson 9. The NRP Provider Card requires renewal every 2 years. Your facility
Simulation 3: Post-term Baby in Labor and Delivery
 Simulation 3: Post-term Baby in Labor and Delivery Opening Scenario (Links to Section 1) You are an evening-shift respiratory therapist in a large hospital with a level III neonatal unit. You are paged
Simulation 3: Post-term Baby in Labor and Delivery Opening Scenario (Links to Section 1) You are an evening-shift respiratory therapist in a large hospital with a level III neonatal unit. You are paged
MODULE VII. Delivery and Immediate Neonatal Care
 MODULE VII Delivery and Immediate Neonatal Care NEONATAL ASPHYXIA About one million deaths per year In Latin America 12% of newborns suffer some degree of asphyxia A major cause of perinatal and neonatal
MODULE VII Delivery and Immediate Neonatal Care NEONATAL ASPHYXIA About one million deaths per year In Latin America 12% of newborns suffer some degree of asphyxia A major cause of perinatal and neonatal
MODULE VII. Delivery and Immediate Neonatal Care
 MODULE VII Delivery and Immediate Neonatal Care NEONATAL ASPHYXIA About one million deaths per year In Latin America 12% of newborns suffer some degree of asphyxia Main cause of perinatal and neonatal
MODULE VII Delivery and Immediate Neonatal Care NEONATAL ASPHYXIA About one million deaths per year In Latin America 12% of newborns suffer some degree of asphyxia Main cause of perinatal and neonatal
1 Pediatric Advanced Life Support Science Update What s New for 2010? 3 CPR. 4 4 Steps of BLS Survey 5 CPR 6 CPR.
 1 Pediatric Advanced Life Support Science Update 2010 2 What s New for 2010? 3 CPR Take no longer than seconds for pulse check Rate at least on per minute (instead of around 100 per minute ) Depth change:
1 Pediatric Advanced Life Support Science Update 2010 2 What s New for 2010? 3 CPR Take no longer than seconds for pulse check Rate at least on per minute (instead of around 100 per minute ) Depth change:
TRAINING NEONATOLOGY SILVANA PARIS
 TRAINING ON NEONATOLOGY SILVANA PARIS RESUSCITATION IN DELIVERY ROOM INTRODUCTION THE GLOBAL RESUSCITATION BURDEN IN NEWBORN 136 MILL NEWBORN BABIES EACH YEAR (WHO WORLD REPORT) 5-8 MILL NEWBORN INFANTS
TRAINING ON NEONATOLOGY SILVANA PARIS RESUSCITATION IN DELIVERY ROOM INTRODUCTION THE GLOBAL RESUSCITATION BURDEN IN NEWBORN 136 MILL NEWBORN BABIES EACH YEAR (WHO WORLD REPORT) 5-8 MILL NEWBORN INFANTS
Neonatal Resuscitation. Dustin Coyle, M.D. Anesthesiology
 Neonatal Resuscitation Dustin Coyle, M.D. Anesthesiology Recognize complications Maternal-fetal factors Maternal DM PIH Chronic HTN Previous stillbirth Rh sensitization Infection Substance abuse/certain
Neonatal Resuscitation Dustin Coyle, M.D. Anesthesiology Recognize complications Maternal-fetal factors Maternal DM PIH Chronic HTN Previous stillbirth Rh sensitization Infection Substance abuse/certain
Neonatal Resuscitation in What is new? How did we get here? Steven Ringer MD PhD Harvard Medical School May 25, 2011
 Neonatal Resuscitation in 2011- What is new? How did we get here? Steven Ringer MD PhD Harvard Medical School May 25, 2011 Conflicts I have no actual or potential conflict of interest in relation to this
Neonatal Resuscitation in 2011- What is new? How did we get here? Steven Ringer MD PhD Harvard Medical School May 25, 2011 Conflicts I have no actual or potential conflict of interest in relation to this
A SYNOPSIS BY ILCOR PEDIATRIC TASK FORCE. Pediatric Basic Life Support, Pediatric Advanced Life Support and Neonatal Resuscitation 2015
 Vol. 2 - No.4 October - December 2015 83 Vol. 2 - No.4 October - December 2015 84 There is new evidence that when treating pediatric septic shock in specific settings, the use of restricted volume of isotonic
Vol. 2 - No.4 October - December 2015 83 Vol. 2 - No.4 October - December 2015 84 There is new evidence that when treating pediatric septic shock in specific settings, the use of restricted volume of isotonic
ENDOTRACHEAL INTUBATION POLICY
 POLICY Indications: Ineffective ventilation with mask and t-piece, or mask and bag technique Inability to maintain a patent airway Need or anticipation of need for prolonged ventilation Need for endotracheal
POLICY Indications: Ineffective ventilation with mask and t-piece, or mask and bag technique Inability to maintain a patent airway Need or anticipation of need for prolonged ventilation Need for endotracheal
Resuscitation efforts for Mom & Baby
 Resuscitation efforts for Mom & Baby Beth Ann Clayton, CRNA, MS AmSol Obstetric Anesthesia CRNA Educator Obstetric Anesthesia Clinical Coordinator Mercy Health-Fairfield Hospital Assistant Professor, University
Resuscitation efforts for Mom & Baby Beth Ann Clayton, CRNA, MS AmSol Obstetric Anesthesia CRNA Educator Obstetric Anesthesia Clinical Coordinator Mercy Health-Fairfield Hospital Assistant Professor, University
Steven Ringer MD PhD April 5, 2011
 Steven Ringer MD PhD April 5, 2011 Disclaimer Mead Johnson sponsors programs such as this to give healthcare professionals access to scientific and educational information provided by experts. The presenter
Steven Ringer MD PhD April 5, 2011 Disclaimer Mead Johnson sponsors programs such as this to give healthcare professionals access to scientific and educational information provided by experts. The presenter
Neonatal/Pediatric Cardiopulmonary Care
 Neonatal/Pediatric Cardiopulmonary Care Resuscitation 2 When To Resuscitate Need usually related Combination of Can occur in 3 Causes of Fetal Asphyxia 1 4 Apnea Hypoxia Stimulates chemoreceptors & baroreceptors
Neonatal/Pediatric Cardiopulmonary Care Resuscitation 2 When To Resuscitate Need usually related Combination of Can occur in 3 Causes of Fetal Asphyxia 1 4 Apnea Hypoxia Stimulates chemoreceptors & baroreceptors
Guslihan Dasa Tjipta Division of Perinatology Department of Child Health Medical School University of Sumatera Utara
 Guslihan Dasa Tjipta Division of Perinatology Department of Child Health Medical School University of Sumatera Utara 1 Definition Perinatal asphyxia is a fetus/newborn, due to: is an insult to the Lack
Guslihan Dasa Tjipta Division of Perinatology Department of Child Health Medical School University of Sumatera Utara 1 Definition Perinatal asphyxia is a fetus/newborn, due to: is an insult to the Lack
Pediatric Advanced Life Support Overview Judy Haluka BS, RCIS, EMT-P
 Pediatric Advanced Life Support Overview 2006 Judy Haluka BS, RCIS, EMT-P General Our Database is lacking in pediatrics Pediatrics are DIFFERENT than Adults not just smaller The same procedure may require
Pediatric Advanced Life Support Overview 2006 Judy Haluka BS, RCIS, EMT-P General Our Database is lacking in pediatrics Pediatrics are DIFFERENT than Adults not just smaller The same procedure may require
These signs should lead to the administration of high concentrations of
 Hypoxic-ischemic encephalopathy (HIE); (cont.) Clinical manifestations; *Intrauterine; growth restriction and increased vascular resistances may be the st manifestation of fetal hypoxia. *During labor;
Hypoxic-ischemic encephalopathy (HIE); (cont.) Clinical manifestations; *Intrauterine; growth restriction and increased vascular resistances may be the st manifestation of fetal hypoxia. *During labor;
HeartCode PALS. PALS Actions Overview > Legend. Contents
 HeartCode PALS PALS Actions Overview > Legend Action buttons (round buttons) Clicking a round button initiates an action. Clicking this button, for example, checks the child s carotid pulse. Menu buttons
HeartCode PALS PALS Actions Overview > Legend Action buttons (round buttons) Clicking a round button initiates an action. Clicking this button, for example, checks the child s carotid pulse. Menu buttons
Surfactant Administration
 Approved by: Surfactant Administration Gail Cameron Senior Director Operations, Maternal, Neonatal & Child Health Programs Dr. Paul Byrne Medical Director, Neonatology Neonatal Policy & Procedures Manual
Approved by: Surfactant Administration Gail Cameron Senior Director Operations, Maternal, Neonatal & Child Health Programs Dr. Paul Byrne Medical Director, Neonatology Neonatal Policy & Procedures Manual
PALS Case Scenario Testing Checklist Respiratory Case Scenario 1 Upper Airway Obstruction
 Respiratory Case Scenario 1 Upper Airway Obstruction Directs administration of 100% oxygen or supplementary oxygen as needed to support oxygenation Identifies signs and symptoms of upper airway obstruction
Respiratory Case Scenario 1 Upper Airway Obstruction Directs administration of 100% oxygen or supplementary oxygen as needed to support oxygenation Identifies signs and symptoms of upper airway obstruction
Neonatal Resuscitation
 Neonatal Resuscitation High Risk Deliveries A person trained in neonatal resuscitation is usually called to be present for the following deliveries: 1. Antepartum factors Maternal diabetes Pregnancy induced
Neonatal Resuscitation High Risk Deliveries A person trained in neonatal resuscitation is usually called to be present for the following deliveries: 1. Antepartum factors Maternal diabetes Pregnancy induced
Infection. Risk factor for infection ACoRN alerting sign with * Clinical deterioration. Problem List. Respiratory. Cardiovascular
 The ACoRN Process Baby at risk Unwell Risk factors Post-resuscitation requiring stabilization Resuscitation Ineffective breathing Heart rate < 100 bpm Central cyanosis Support Infection Risk factor for
The ACoRN Process Baby at risk Unwell Risk factors Post-resuscitation requiring stabilization Resuscitation Ineffective breathing Heart rate < 100 bpm Central cyanosis Support Infection Risk factor for
Chain of Survival. Highlights of 2010 American Heart Guidelines CPR
 Highlights of 2010 American Heart Guidelines CPR Compressions rate of at least 100/min. allow for complete chest recoil Adult CPR depth of at least 2 inches Child/Infant CPR depth of 1/3 anterior/posterior
Highlights of 2010 American Heart Guidelines CPR Compressions rate of at least 100/min. allow for complete chest recoil Adult CPR depth of at least 2 inches Child/Infant CPR depth of 1/3 anterior/posterior
NEONATOLOGY Healthy newborn. Neonatal sequelaes
 NEONATOLOGY Healthy newborn. Neonatal sequelaes Ágnes Harmath M.D. Ph.D. senior lecturer 11. November 2016. Tasks of the neonatologist Prenatal diagnosed condition Inform parents, preparation of necessary
NEONATOLOGY Healthy newborn. Neonatal sequelaes Ágnes Harmath M.D. Ph.D. senior lecturer 11. November 2016. Tasks of the neonatologist Prenatal diagnosed condition Inform parents, preparation of necessary
Paediatric Resuscitation. EMS Rounds Gurinder Sangha MD Paediatric Emergency Fellow June 18, 2009
 Paediatric Resuscitation EMS Rounds Gurinder Sangha MD Paediatric Emergency Fellow June 18, 2009 Essentials of Resuscitation Airway Breathing Circulation AIRWAY Differences in Paediatric Airway Shorter
Paediatric Resuscitation EMS Rounds Gurinder Sangha MD Paediatric Emergency Fellow June 18, 2009 Essentials of Resuscitation Airway Breathing Circulation AIRWAY Differences in Paediatric Airway Shorter
2. General Cardiac Arrest Protocol Medical Newborn/Neonatal. Protocol 8-3 Resuscitation 4. Medical Supraventricular
 PEDIATRIC CARDIAC SECTION: Pediatric Cardiovascular Emergencies REVISED: 06/2017 Section 8 1. Cardiac Arrest Unknown Rhythm (i.e. Protocol 8-1 BLS) 2. General Cardiac Arrest Protocol 8-2 3. Medical Newborn/Neonatal
PEDIATRIC CARDIAC SECTION: Pediatric Cardiovascular Emergencies REVISED: 06/2017 Section 8 1. Cardiac Arrest Unknown Rhythm (i.e. Protocol 8-1 BLS) 2. General Cardiac Arrest Protocol 8-2 3. Medical Newborn/Neonatal
Learning Station Competency Checklists
 Learning Station Competency Checklists Cardiac Arrest: Shockable Rhythm Team Dynamics Practice Demonstrates effective team dynamics (see, below) Performs manual maneuvers to open airway* Initiates assisted
Learning Station Competency Checklists Cardiac Arrest: Shockable Rhythm Team Dynamics Practice Demonstrates effective team dynamics (see, below) Performs manual maneuvers to open airway* Initiates assisted
SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE
 SARASOTA MEMORIAL HOSPITAL TITLE: NURSING PROCEDURE Management, Monitoring & Documentation of a Clinically Significant Cardiopulmonary Event (CSCPE) (NUR47) DATE: REVIEWED: PAGES: 9/09 9/17 1 of 6 PS1094
SARASOTA MEMORIAL HOSPITAL TITLE: NURSING PROCEDURE Management, Monitoring & Documentation of a Clinically Significant Cardiopulmonary Event (CSCPE) (NUR47) DATE: REVIEWED: PAGES: 9/09 9/17 1 of 6 PS1094
GUIDELINE PHYSIOLOGY OF BIRTH ASPHYXIA
 GUIDELINE PHYSIOLOGY OF BIRTH ASPHYXIA The newborn is not an adult, nor a child. In people of all ages, death can occur from a failure of breathing and / or circulation. The interventions required to aid
GUIDELINE PHYSIOLOGY OF BIRTH ASPHYXIA The newborn is not an adult, nor a child. In people of all ages, death can occur from a failure of breathing and / or circulation. The interventions required to aid
Presented By : Kamlah Olaimat
 Presented By : Kamlah Olaimat 18\7\2010 Transient Tachpnea of the Definition:- newborn (TTN) TTN is a benign disease of near term or term infant who display respiratory distress shortly after delivery.
Presented By : Kamlah Olaimat 18\7\2010 Transient Tachpnea of the Definition:- newborn (TTN) TTN is a benign disease of near term or term infant who display respiratory distress shortly after delivery.
Pediatric Shock. Hypovolemia. Sepsis. Most common cause of pediatric shock Small blood volumes (80cc/kg)
") Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
ACoRN Workbook 2012 Update
 ACoRN Neonatal Society Société néonatale ACoRN www.acornprogram.net A Canadian non-profit Society Vancouver, British Columbia ACoRN Workbook 2012 Update Name: The ACoRN Process The Resuscitation Sequence
ACoRN Neonatal Society Société néonatale ACoRN www.acornprogram.net A Canadian non-profit Society Vancouver, British Columbia ACoRN Workbook 2012 Update Name: The ACoRN Process The Resuscitation Sequence
Review of Neonatal Respiratory Problems
 Review of Neonatal Respiratory Problems Respiratory Distress Occurs in about 7% of infants Clinical presentation includes: Apnea Cyanosis Grunting Inspiratory stridor Nasal flaring Poor feeding Tachypnea
Review of Neonatal Respiratory Problems Respiratory Distress Occurs in about 7% of infants Clinical presentation includes: Apnea Cyanosis Grunting Inspiratory stridor Nasal flaring Poor feeding Tachypnea
Stabilization of the Newborn for Transport. Relevant Disclosure. Learning Objectives
 Stabilization of the Newborn for Transport Arlen Foulks, DO FAAP FACOP Medical Director, CCMH Level II NICU Medical Director, NeoFlight Assistant Professor of Pediatrics Neonatal Perinatal Medicine Section,
Stabilization of the Newborn for Transport Arlen Foulks, DO FAAP FACOP Medical Director, CCMH Level II NICU Medical Director, NeoFlight Assistant Professor of Pediatrics Neonatal Perinatal Medicine Section,
CARDIAC EMERGENCIES Other Cardiac Dysrhythmias C9
 CARDIAC EMERGENCIES Other Cardiac Dysrhythmias C9 ATRIAL FLUTTER Variable rate depending on block. Atrial rate between 250-350, saw-tooth pattern. (see Appendix B for energy settings for bi-phasic low
CARDIAC EMERGENCIES Other Cardiac Dysrhythmias C9 ATRIAL FLUTTER Variable rate depending on block. Atrial rate between 250-350, saw-tooth pattern. (see Appendix B for energy settings for bi-phasic low
Appendix D An unresponsive patient with shallow, gasping breaths at a rate of six per minute requires:
 Answer Key Appendix D-2 1. An unresponsive patient with shallow, gasping breaths at a rate of six per minute requires: a. oxygen given via nasal cannula b. immediate transport to a medical facility c.
Answer Key Appendix D-2 1. An unresponsive patient with shallow, gasping breaths at a rate of six per minute requires: a. oxygen given via nasal cannula b. immediate transport to a medical facility c.
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device
 I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel
Nassau Regional Emergency Medical Services. Advanced Life Support Pediatric Protocol Manual
 Nassau Regional Emergency Medical Services Advanced Life Support Pediatric Protocol Manual 2014 PEDIATRIC ADVANCED LIFE SUPPORT PROTOCOLS TABLE OF CONTENTS Approved Effective Newborn Resuscitation P 1
Nassau Regional Emergency Medical Services Advanced Life Support Pediatric Protocol Manual 2014 PEDIATRIC ADVANCED LIFE SUPPORT PROTOCOLS TABLE OF CONTENTS Approved Effective Newborn Resuscitation P 1
Preface. The ACoRN Neonatal Society. ACoRN xiii
 Preface For most health professionals, few events are more challenging or stressful than caring for a sick or preterm baby. It is therefore not surprising that the management and stabilization of these
Preface For most health professionals, few events are more challenging or stressful than caring for a sick or preterm baby. It is therefore not surprising that the management and stabilization of these
Pedi-Cap CO 2 detector
 Pedi-Cap CO 2 detector Presentation redeveloped for this program by Rosemarie Boland from an original presentation by Johnston, Adams & Stewart, (2006) Background Clinical methods of endotracheal tube
Pedi-Cap CO 2 detector Presentation redeveloped for this program by Rosemarie Boland from an original presentation by Johnston, Adams & Stewart, (2006) Background Clinical methods of endotracheal tube
Objectives. Birth Depression Management. Birth Depression Terms
 Objectives Birth Depression Management Regional Perinatal Outreach Program 2016 Understand the terms and the clinical characteristics of birth depression. Be familiar with the evidence behind therapeutic
Objectives Birth Depression Management Regional Perinatal Outreach Program 2016 Understand the terms and the clinical characteristics of birth depression. Be familiar with the evidence behind therapeutic
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
1 Chapter 40 Advanced Airway Management 2 Advanced Airway Management The advanced airway management techniques discussed in this chapter are to
 1 Chapter 40 Advanced Airway Management 2 Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only. In
1 Chapter 40 Advanced Airway Management 2 Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only. In
ISPUB.COM. The Use of LMA in Newborn Resuscitation. R Vadhera INTRODUCTION VENTILATION
 ISPUB.COM The Internet Journal of Anesthesiology Volume 1 Number 4 The Use of LMA in Newborn Resuscitation R Vadhera Citation R Vadhera. The Use of LMA in Newborn Resuscitation. The Internet Journal of
ISPUB.COM The Internet Journal of Anesthesiology Volume 1 Number 4 The Use of LMA in Newborn Resuscitation R Vadhera Citation R Vadhera. The Use of LMA in Newborn Resuscitation. The Internet Journal of
Other methods for maintaining the airway (not definitive airway as still unprotected):
:") Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
Provide guidelines for the management of mechanical ventilation in infants <34 weeks gestation.
 Page 1 of 5 PURPOSE: Provide guidelines for the management of mechanical ventilation in infants
Page 1 of 5 PURPOSE: Provide guidelines for the management of mechanical ventilation in infants
Pediatric CPR. Mustafa SERİNKEN MD Professor of Emergency Medicine, Pamukkale University, TURKEY
 Pediatric CPR Mustafa SERİNKEN MD Professor of Emergency Medicine, Pamukkale University, TURKEY What are the differences? Normal limits ADULT CARDIOPULMONARY ARREST CAUSES INFANTS AND CHILDREN İschemic
Pediatric CPR Mustafa SERİNKEN MD Professor of Emergency Medicine, Pamukkale University, TURKEY What are the differences? Normal limits ADULT CARDIOPULMONARY ARREST CAUSES INFANTS AND CHILDREN İschemic
Chapter 40 Advanced Airway Management
 1 2 3 4 5 Chapter 40 Advanced Airway Management Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only.
1 2 3 4 5 Chapter 40 Advanced Airway Management Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only.
table of contents pediatric treatment guidelines
 table of contents pediatric treatment guidelines P1 PEDIATRIC PATIENT CARE...70 P2 APPARENT LIFE-THREATENING EVENT (ALTE)...71 P3 CARDIAC ARREST INITIAL CARE AND CPR...72 73 P4 NEONATAL CARE AND RESUSCITATION...74
table of contents pediatric treatment guidelines P1 PEDIATRIC PATIENT CARE...70 P2 APPARENT LIFE-THREATENING EVENT (ALTE)...71 P3 CARDIAC ARREST INITIAL CARE AND CPR...72 73 P4 NEONATAL CARE AND RESUSCITATION...74
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 14 Practical Anesthesia Key Points 2 14.1 General Anesthesia Have a clear plan before starting anesthesia Never use an unfamiliar anesthetic technique in an emergency
Surgical Care at the District Hospital 1 14 Practical Anesthesia Key Points 2 14.1 General Anesthesia Have a clear plan before starting anesthesia Never use an unfamiliar anesthetic technique in an emergency
Anatomy and Physiology. The airways can be divided in to parts namely: The upper airway. The lower airway.
 Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Insight. Resuscitation Guidelines Summary of Key Changes
 Insight Resuscitation Guidelines 2015 - Summary of Key Changes Introduction Our 2020 Vision is to help save 500,000 more lives every year and therefore it seems fitting that we should help disseminate
Insight Resuscitation Guidelines 2015 - Summary of Key Changes Introduction Our 2020 Vision is to help save 500,000 more lives every year and therefore it seems fitting that we should help disseminate
ADVANCED AIRWAY MANAGEMENT
 The Advanced Airway Management protocol should be used on all patients requiring advanced airway management procedures. This protocol is divided into three sections the Crash Airway Algorithm, the Rapid
The Advanced Airway Management protocol should be used on all patients requiring advanced airway management procedures. This protocol is divided into three sections the Crash Airway Algorithm, the Rapid
McMaster Neonatal Skills Workshop Procedure Pearls
 McMaster Neonatal Skills Workshop Procedure Pearls November 2, 2016 Image from: www.prweb.com Procedures www.laerdal.com www.gaumard.com www.rch.org.au www.laerdal.com ekja.org NRP Epinephrine: 0.1ml/kg
McMaster Neonatal Skills Workshop Procedure Pearls November 2, 2016 Image from: www.prweb.com Procedures www.laerdal.com www.gaumard.com www.rch.org.au www.laerdal.com ekja.org NRP Epinephrine: 0.1ml/kg
PEMSS PROTOCOLS INVASIVE PROCEDURES
 PEMSS PROTOCOLS INVASIVE PROCEDURES Panhandle Emergency Medical Services System SURGICAL AND NEEDLE CRICOTHYROTOMY Inability to intubate is the primary indication for creating an artificial airway. Care
PEMSS PROTOCOLS INVASIVE PROCEDURES Panhandle Emergency Medical Services System SURGICAL AND NEEDLE CRICOTHYROTOMY Inability to intubate is the primary indication for creating an artificial airway. Care
PALS Review 2015 Guidelines
 PALS Review 2015 Guidelines BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. 1. Scene Safety 2. Establish Unresponsiveness 3. Check for breathing if absent or agonal (No
PALS Review 2015 Guidelines BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. 1. Scene Safety 2. Establish Unresponsiveness 3. Check for breathing if absent or agonal (No
ITLS Pediatric Provider Course Basic Pre-Test
 ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
Advanced Airway Management PRESENTED BY: JOSIAH POIRIER RN, JOHN GRUBER FP-C
 Advanced Airway Management PRESENTED BY: JOSIAH POIRIER RN, JOHN GRUBER FP-C Advanced Airway Objectives Advanced airway management is a relatively low frequency, high risk intervention. The following education
Advanced Airway Management PRESENTED BY: JOSIAH POIRIER RN, JOHN GRUBER FP-C Advanced Airway Objectives Advanced airway management is a relatively low frequency, high risk intervention. The following education
Guidelines and Best Practices for Vapotherm High Velocity Nasal Insufflation (Hi-VNI ) NICU POCKET GUIDE
 NICU POCKET GUIDE") Guidelines and Best Practices for Vapotherm High Velocity Nasal Insufflation (Hi-VNI ) TM NICU POCKET GUIDE Patient Selection Diagnoses Patient presents with one or more of the following symptoms: These
Guidelines and Best Practices for Vapotherm High Velocity Nasal Insufflation (Hi-VNI ) TM NICU POCKET GUIDE Patient Selection Diagnoses Patient presents with one or more of the following symptoms: These
Pediatrics 1 Neonatal Resuscitation Pediatric Assessment Airway Management. Neonatology. Topics. EMT Paramedic / Critical Refresher Session # 22
 EMT Paramedic / Critical Refresher Session # 22 Pediatrics 1 Neonatal Resuscitation Pediatric Assessment Airway Management 1 Neonatology 2 Topics Newborns & Neonates High Risk Newborn Patients APGAR Scoring
EMT Paramedic / Critical Refresher Session # 22 Pediatrics 1 Neonatal Resuscitation Pediatric Assessment Airway Management 1 Neonatology 2 Topics Newborns & Neonates High Risk Newborn Patients APGAR Scoring
Non-Invasive Monitoring
 Grey Nuns and Misericordia Community Hospital Approved by: Non-Invasive Monitoring Neonatal Policy & Procedures Manual : Assessment : Oct 2015 Date Effective Oct 2015 Gail Cameron Senior Director Operations,
Grey Nuns and Misericordia Community Hospital Approved by: Non-Invasive Monitoring Neonatal Policy & Procedures Manual : Assessment : Oct 2015 Date Effective Oct 2015 Gail Cameron Senior Director Operations,
PALS NEW GUIDELINES 2010
 PALS NEW GUIDELINES 2010 DR WALEED ALAMRI PEDIATRIC EMERGENCY CONSULTANT FEB 24, 2011 Pediatric Basic Life Support Change in CPR Sequence (C-A-B Rather Than A-B-C) 2010 (New): Initiate CPR for infants
PALS NEW GUIDELINES 2010 DR WALEED ALAMRI PEDIATRIC EMERGENCY CONSULTANT FEB 24, 2011 Pediatric Basic Life Support Change in CPR Sequence (C-A-B Rather Than A-B-C) 2010 (New): Initiate CPR for infants
Subspecialty Rotation: Anesthesia
 Subspecialty Rotation: Anesthesia Faculty: John Heaton, M.D. GOAL: Maintenance of Airway Patency and Oxygenation. Recognize and manage upper airway obstruction and desaturation. Recognize and manage upper
Subspecialty Rotation: Anesthesia Faculty: John Heaton, M.D. GOAL: Maintenance of Airway Patency and Oxygenation. Recognize and manage upper airway obstruction and desaturation. Recognize and manage upper
This interdisciplinary clinical support document provides guidelines for the safe establishment of an artificial airway.
 PURPOSE This interdisciplinary clinical support document provides guidelines for the safe establishment of an artificial airway. POLICY STATEMENTS Endotracheal intubation will be performed by the Most
PURPOSE This interdisciplinary clinical support document provides guidelines for the safe establishment of an artificial airway. POLICY STATEMENTS Endotracheal intubation will be performed by the Most
2015 Interim Training Materials
 2015 Interim Training Materials ACLS Manual and ACLS EP Manual Comparison Chart Assessment sequence Manual, Part 2: The Systematic Approach, and Part BLS Changes The HCP should check for response while
2015 Interim Training Materials ACLS Manual and ACLS EP Manual Comparison Chart Assessment sequence Manual, Part 2: The Systematic Approach, and Part BLS Changes The HCP should check for response while
INTUBATION/RSI. PURPOSE: A. To facilitate secure, definitive control of the airway by endotracheal intubation in an expeditious and safe manner
 Manual: LifeLine Patient Care Protocols Section: Adult/Pediatrics Protocol #: AP1-009 Approval Date: 03/01/2018 Effective Date: 03/05/2018 Revision Due Date: 12/01/2018 INTUBATION/RSI PURPOSE: A. To facilitate
Manual: LifeLine Patient Care Protocols Section: Adult/Pediatrics Protocol #: AP1-009 Approval Date: 03/01/2018 Effective Date: 03/05/2018 Revision Due Date: 12/01/2018 INTUBATION/RSI PURPOSE: A. To facilitate
NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY
 & COOLING THERAPY") Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
** SURFACTANT THERAPY**
 ** SURFACTANT THERAPY** Full Title of Guideline: Surfactant Therapy Author (include email and role): Stephen Wardle (V4) Reviewed by Dushyant Batra Consultant Neonatologist Division & Speciality: Division:
** SURFACTANT THERAPY** Full Title of Guideline: Surfactant Therapy Author (include email and role): Stephen Wardle (V4) Reviewed by Dushyant Batra Consultant Neonatologist Division & Speciality: Division:
Hyaline membrane disease. By : Dr. Ch Sarishma Peadiatric Pg
 Hyaline membrane disease By : Dr. Ch Sarishma Peadiatric Pg Also called Respiratory distress syndrome. It occurs primarily in premature infants; its incidence is inversely related to gestational age and
Hyaline membrane disease By : Dr. Ch Sarishma Peadiatric Pg Also called Respiratory distress syndrome. It occurs primarily in premature infants; its incidence is inversely related to gestational age and
Prehospital Care Bundles
 Prehospital s The MLREMS Prehospital s have been created to provide a simple framework to help EMS providers identify the most critical elements when caring for a patient. These bundles do not replace
Prehospital s The MLREMS Prehospital s have been created to provide a simple framework to help EMS providers identify the most critical elements when caring for a patient. These bundles do not replace
Pediatric Cardiac Arrest General
 Date: November 15, 2012 Page 1 of 5 Pediatric Cardiac Arrest General This protocol should be followed for all pediatric cardiac arrests. If an arrest is of a known traumatic origin refer to the Dead on
Date: November 15, 2012 Page 1 of 5 Pediatric Cardiac Arrest General This protocol should be followed for all pediatric cardiac arrests. If an arrest is of a known traumatic origin refer to the Dead on
ILCOR ADVISORY STATEMENT: RESUSCITATION OF THE NEWLY BORN INFANT. An Advisory Statement From the Pediatric Working Group of the
 ILCOR ADVISORY STATEMENT: RESUSCITATION OF THE NEWLY BORN INFANT An Advisory Statement From the Pediatric Working Group of the International Liaison Committee on Resuscitation John Kattwinkel, MD* ; Susan
ILCOR ADVISORY STATEMENT: RESUSCITATION OF THE NEWLY BORN INFANT An Advisory Statement From the Pediatric Working Group of the International Liaison Committee on Resuscitation John Kattwinkel, MD* ; Susan
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of
 Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Airway Management Essentials Self-Study Guide
 Airway Management Essentials Self-Study Guide Fourth Quarter 2010 Self-Study Guide Learning Objectives Cognitive Domain 1. Describe the various conditions that cause concern during treatment in the field
Airway Management Essentials Self-Study Guide Fourth Quarter 2010 Self-Study Guide Learning Objectives Cognitive Domain 1. Describe the various conditions that cause concern during treatment in the field
SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC
 SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC The following is a summary of the key issues and changes in the AHA 2010 Guidelines for Cardiopulmonary Resuscitation (CPR) and Emergency Cardiac
SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC The following is a summary of the key issues and changes in the AHA 2010 Guidelines for Cardiopulmonary Resuscitation (CPR) and Emergency Cardiac
Waitin In The Wings. Esophageal/Tracheal Double Lumen Airway (Combitube ) Indications and Use for the Pre-Hospital Provider
 Indications and Use for the Pre-Hospital Provider") Waitin In The Wings Esophageal/Tracheal Double Lumen Airway (Combitube ) Indications and Use for the Pre-Hospital Provider 1 CombiTube Kit General Description The CombiTube is A double-lumen tube with
Waitin In The Wings Esophageal/Tracheal Double Lumen Airway (Combitube ) Indications and Use for the Pre-Hospital Provider 1 CombiTube Kit General Description The CombiTube is A double-lumen tube with
Basic Airway Management
 Basic Airway Management Dr. Madhurita Singh, Assoc. Professor, Dept. of Critical Care, CMC Vellore. This is the first module in a series on management of airway and ventilation in critically ill patients.
Basic Airway Management Dr. Madhurita Singh, Assoc. Professor, Dept. of Critical Care, CMC Vellore. This is the first module in a series on management of airway and ventilation in critically ill patients.
COMMISSION ON ACCREDITATION FOR RESPIRATORY CARE TMC DETAILED CONTENT OUTLINE COMPARISON
 A. Evaluate Data in the Patient Record I. PATIENT DATA EVALUATION AND RECOMMENDATIONS 1. Patient history e.g., admission data orders medications progress notes DNR status / advance directives social history
A. Evaluate Data in the Patient Record I. PATIENT DATA EVALUATION AND RECOMMENDATIONS 1. Patient history e.g., admission data orders medications progress notes DNR status / advance directives social history
Code Blue III PLUS. Emergency Care Simulators
 Code Blue III PLUS Emergency Care Simulators Our Code Blue III system teaches ALS skills using realistic code scenarios. Each step you take is monitored by software providing important feedback, not only
Code Blue III PLUS Emergency Care Simulators Our Code Blue III system teaches ALS skills using realistic code scenarios. Each step you take is monitored by software providing important feedback, not only
Simulation 08: Cyanotic Preterm Infant in Respiratory Distress
 Flow Chart Simulation 08: Cyanotic Preterm Infant in Respiratory Distress Opening Scenario Section 1 Type: DM As staff therapist assigned to a Level 2 NICU in a 250 bed rural medical center you are called
Flow Chart Simulation 08: Cyanotic Preterm Infant in Respiratory Distress Opening Scenario Section 1 Type: DM As staff therapist assigned to a Level 2 NICU in a 250 bed rural medical center you are called
The ALS Algorithm and Post Resuscitation Care
 The ALS Algorithm and Post Resuscitation Care CET - Ballarat Health Services Valid from 1 st July 2018 to 30 th June 2020 2 Defibrillation Produces simultaneous mass depolarisation of myocardial cells
The ALS Algorithm and Post Resuscitation Care CET - Ballarat Health Services Valid from 1 st July 2018 to 30 th June 2020 2 Defibrillation Produces simultaneous mass depolarisation of myocardial cells
10/13/2017. Newborn Care. Objectives. Cardiac Anatomy. Managing Transitional Physiology
 Newborn Care Managing Transitional Physiology Mary Coughlin MS, NNP, RNC-E President and Founder Caring Essentials Collaborative Boston, MA Objectives Upon completion of the learning session participants
Newborn Care Managing Transitional Physiology Mary Coughlin MS, NNP, RNC-E President and Founder Caring Essentials Collaborative Boston, MA Objectives Upon completion of the learning session participants
Cardiopulmonary Resuscitation in Adults
 Cardiopulmonary Resuscitation in Adults Fatma Özdemir, MD Emergency Deparment of Uludag University Faculty of Medicine OVERVIEW Introduction Pathophysiology BLS algorithm ALS algorithm Post resuscitation
Cardiopulmonary Resuscitation in Adults Fatma Özdemir, MD Emergency Deparment of Uludag University Faculty of Medicine OVERVIEW Introduction Pathophysiology BLS algorithm ALS algorithm Post resuscitation
The Blue Baby. Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin
 The Blue Baby Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin Session Structure Definitions and assessment of cyanosis Causes of blue baby Structured approach to assessing
The Blue Baby Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin Session Structure Definitions and assessment of cyanosis Causes of blue baby Structured approach to assessing
Advanced Airway Management
 CHAPTER 37 Advanced Airway Management Airway Anatomy and Physiology Review Respiratory System: The Airway Respiratory System (Supine) Physiology: Factors of Adequate Breathing Functioning brainstem Open
CHAPTER 37 Advanced Airway Management Airway Anatomy and Physiology Review Respiratory System: The Airway Respiratory System (Supine) Physiology: Factors of Adequate Breathing Functioning brainstem Open
Scope This guideline is aimed at all Health care professionals involved in the care of infants within the Neonatal Service.
 Management of Newborn Infants born through Meconium-stained liquor University Hospitals of Leicester NHS NHS Trust March 2018 March 2021 Scope This guideline is aimed at all Health care professionals involved
Management of Newborn Infants born through Meconium-stained liquor University Hospitals of Leicester NHS NHS Trust March 2018 March 2021 Scope This guideline is aimed at all Health care professionals involved
Duct Dependant Congenital Heart Disease
 Children s Acute Transport Service Clinical Guidelines Duct Dependant Congenital Heart Disease This guideline has been agreed by both NTS & CATS Document Control Information Author CATS/NTS Author Position
Children s Acute Transport Service Clinical Guidelines Duct Dependant Congenital Heart Disease This guideline has been agreed by both NTS & CATS Document Control Information Author CATS/NTS Author Position
Pediatric advanced life support. Management of decreased conscious level in children. Virgi ija Žili skaitė 2017
 Pediatric advanced life support. Management of decreased conscious level in children Virgi ija Žili skaitė 2017 Life threatening conditions: primary assessment, differential diagnostics and emergency care.
Pediatric advanced life support. Management of decreased conscious level in children Virgi ija Žili skaitė 2017 Life threatening conditions: primary assessment, differential diagnostics and emergency care.
The Pediatric Patient. Morgen Bernius, MD NCEMS Conference February 24, 2007
 The Pediatric Patient Morgen Bernius, MD NCEMS Conference February 24, 2007 Rule #1: Everyone Loves the Pediatric Patient Pediatrics in EMS Approximately 10% of all EMS treatment is for children younger
The Pediatric Patient Morgen Bernius, MD NCEMS Conference February 24, 2007 Rule #1: Everyone Loves the Pediatric Patient Pediatrics in EMS Approximately 10% of all EMS treatment is for children younger
Volume Guarantee Initiation and ongoing clinical management of an infant supported by Volume Guarantee A Case Study
 D-32084-2011 Volume Guarantee Initiation and ongoing clinical management of an infant supported by Volume Guarantee A Case Study Robert DiBlasi RRT-NPS, FAARC Respiratory Care Manager of Research & Quality
D-32084-2011 Volume Guarantee Initiation and ongoing clinical management of an infant supported by Volume Guarantee A Case Study Robert DiBlasi RRT-NPS, FAARC Respiratory Care Manager of Research & Quality
Practical Application of CPAP
 CHAPTER 3 Practical Application of CPAP Dr. Srinivas Murki Neonatologist Fernadez Hospital, Hyderabad. A.P. Practical Application of CPAP Continuous positive airway pressure (CPAP) applied to premature
CHAPTER 3 Practical Application of CPAP Dr. Srinivas Murki Neonatologist Fernadez Hospital, Hyderabad. A.P. Practical Application of CPAP Continuous positive airway pressure (CPAP) applied to premature
New Zealand Data Sheet. Poractant alfa (Phospholipid fraction of porcine lung) 80 mg/ml
 80 mg/ml") CUROSURF New Zealand Data Sheet Poractant alfa (Phospholipid fraction of porcine lung) 80 mg/ml Presentation Sterile suspension in single-dose vials for intratracheal or intrabronchial administration.
CUROSURF New Zealand Data Sheet Poractant alfa (Phospholipid fraction of porcine lung) 80 mg/ml Presentation Sterile suspension in single-dose vials for intratracheal or intrabronchial administration.
Objectives. Apnea Definition and Pitfalls. Pathophysiology of Apnea. Apnea of Prematurity and hypoxemia episodes 5/18/2015
 Apnea of Prematurity and hypoxemia episodes Deepak Jain MD Care of Sick Newborn Conference May 2015 Objectives Differentiating between apnea and hypoxemia episodes. Pathophysiology Diagnosis of apnea and
Apnea of Prematurity and hypoxemia episodes Deepak Jain MD Care of Sick Newborn Conference May 2015 Objectives Differentiating between apnea and hypoxemia episodes. Pathophysiology Diagnosis of apnea and
CONTINUOUS POSITIVE AIRWAY PRESSURE (CPAP) DEFINITION
 DEFINITION") CONTINUOUS POSITIVE AIRWAY PRESSURE (CPAP) DEFINITION Method of maintaining low pressure distension of lungs during inspiration and expiration when infant breathing spontaneously Benefits Improves oxygenation
CONTINUOUS POSITIVE AIRWAY PRESSURE (CPAP) DEFINITION Method of maintaining low pressure distension of lungs during inspiration and expiration when infant breathing spontaneously Benefits Improves oxygenation